If you’re being featured in on a site named “Afro” years after you started shaving (not bald!), then the ancestors must be showing favor on you. Hope you enjoy the read.
Take control of your health: A common-sense guide to prevention
If you’re being featured in on a site named “Afro” years after you started shaving (not bald!), then the ancestors must be showing favor on you. Hope you enjoy the read.
Take control of your health: A common-sense guide to prevention
1. What is ivermectin? How is it currently used?
In humans, ivermectin is an anti-parasitic medication. Although it’s often called an anti-worming medication, microscopic parasites are completely unrelated to what we think of as worms. They also aren’t at all like viruses, and so it isn’t intuitive to think this medicine could be effective against viruses. Now in animals, it does treat heartworms, but that has nothing to do with treating viruses.
2. How did the medical notion that ivermectin could be used arise?
Many nations without the benefit of COVID-19 vaccines have taken to using experimental drugs in hope of a “cure.” Ivermectin is one such drug. It has been shown to stop growth of COVID-19 cells in an Australian laboratory (meaning in a petri dish, not in humans). However, be reminded that most medicines will do the same at toxic levels. You can’t take toxic levels of medicine to kill COVID-19 without damaging yourself. It’s like the difference between taking a normal dose of Tylenol to treat pain vs. overdosing on higher levels. Somehow, many of the same people skeptical of the mountains of COVID-19 vaccine research or the previous EUA (and current full approval of Pfizer’s vax) are satisfied with data from a petri dish that hasn’t been confirmed in humans or approved by regulatory agencies.
3. Is the ivermectin used in humans the same as is used in animals?
This is where I remind you why FDA approval and regulation of medications is important. The animal preparations of ivermectin contain about 7 times the amount of active ingredient as the human one (remember that horses are about a ton heavier than humans). Do you care about side effects or toxicity? Care about purity of the preparation? I can’t believe I have to say this, but taking medicine formulated for animals is a disaster waiting to happen.
4. What does the research on ivermectin show?
Simply put, with dozens of research studies completed and ongoing, it clear there isn’t sufficient evidence to say this works against COVID-19. However, there was one paper that created quite the fervor. It summarized the results of a clinical trial seeming to show that ivermectin can reduce COVID-19 death rates by more than 90%. Unfortunately, the study was later withdrawn amidst concerns about plagiarism and data manipulation (read: fraud). Sadly, a lot of those excited about the news missed the follow up reporting. It’s of note that Merck, the pharmaceutical maker of ivermectin, says they have found no scientific basis for a potential therapeutic effect against COVID, no meaningful evidence for clinical activity or clinical efficacy in people with COVID, and a concerning lack of safety data in the majority of studies. Read that again: this is from the manufacturer.
5. What does the WHO, FDA and CDC say about ivermectin?
Regulatory agencies around the world are clear and unanimous that there is no current role for ivermectin in the treatment of COVID-19. Here’s a full statement: https://www.fda.gov/…/why-you-should-not-use-ivermectin…
6. Why not try it? Is it dangerous?
That’s now how medicine works. This is a potentially toxic medicine. “Try it and see” isn’t how medicine is prescribed. Besides, ivermectin can cause nausea, vomiting, diarrhea, low blood pressure, allergic reactions, dizziness, problems with balance, seizures, coma, and death. For what it’s worth, it’s now legendary that those taking the animal preparations are literally pooping their pants. Also, even at approved doses, ivermectin can interact with other medications (e.g. blood thinners).
7. How is this happening? If I “followed the money,” who stands to gain from ivermectin being promoted?
If you are familiar with the group called America’s Frontline Doctors, you’ll recognize them as an ongoing source of disinformation, including prior claims that hydroxychloroquine was a miracle cure. More notoriously, they have been offering online consultations to those seeking ivermectin, at a cost of $90 a pop, subsequently connecting the willing to an affiliated pharmacy that would deliver the medicine. By the way, the use of the animal preparations arose from these pharmacies continually being out of stock (monthly prescriptions have increased from 3600 pre-pandemic to over 88,000 in August 2021). That alone is about $8M/month in revenue to perpetrate a fraud, as the saying goes.


I’m quite conflicted. From multiple angles, I am seeing both national and African American communities being ravaged by COVID-19. I am also seeing both gripped by multiple considerations that prevent achievable progress, and admittedly in both examples, these considerations seem out of the control of those affected. My observations aren’t meant to judge but to enlighten. I believe in a fault in your right to decide how you live and die.
Americans fiercely guard freedom, individualism and choice. For many, these are values that define life, liberty and the pursuit of happiness. In the midst of a pandemic, that too often means a willingness to prioritize actions not in the national or (one would think) self-interest. However, the point of health self-empowerment is people do get to be educated consumers, appreciating that choices have consequences. Unfortunately, that level of selfishness can create downstream havoc on the most vulnerable citizens. The African American community has legitimate concerns related to institutional racism at the hands of the medical establishment. This has ranged from lack of access, unequal quality of care, and higher costs than the general population to outright victimization as the subjects of medical experimentation. There is no fair way to criticize any African American who is hesitant about engaging the medical establishment. This trepidation has translated into a willingness to rely on herbal medicines and home remedies instead of physician prescribed regimens. It means lower rates of vaccine usage and a willingness to roll the dice on surviving known threats when clinically demonstrable options exist. You may not want to hear it or believe it, but these experiences reflect parallels than converge in the production of suboptimal outcomes. The performance of the US on the world stage is shockingly bad, as we lead the world in cases and deaths. African Americans again suffer disproportionately from COVID-19. Again: both external and self-imposed decisions contribute to these health care disparities.
Sadly, the way out in both examples is clear, but the implementation of best practice strategies is a challenge that seems more elusive that our hands are able to grab. As the months roll by and deaths accrue, it will be interesting to see when and if the lightbulbs finally go off and our communities stop being governed by fear (legitimate and not) and priorities other than health. The ongoing question is when will we start taking charge of the conditions that cause that fear and relegation of health to a secondary consideration in our lives? I hope it’s soon across the board. Lives are in the balance.

This Straight No Chaser addresses next steps after a diagnosis of COVID-19. The post addresses those with mild or no symptoms. There have been well over 3.4 million Americans diagnosed with COVID-19. Are you one? What did you do next? If not, do you know what to do next?
Here’s a checklist of recommended next steps after a diagnosis of COVID-19. If you’re following these, both you and your contacts will likely come through it ok.
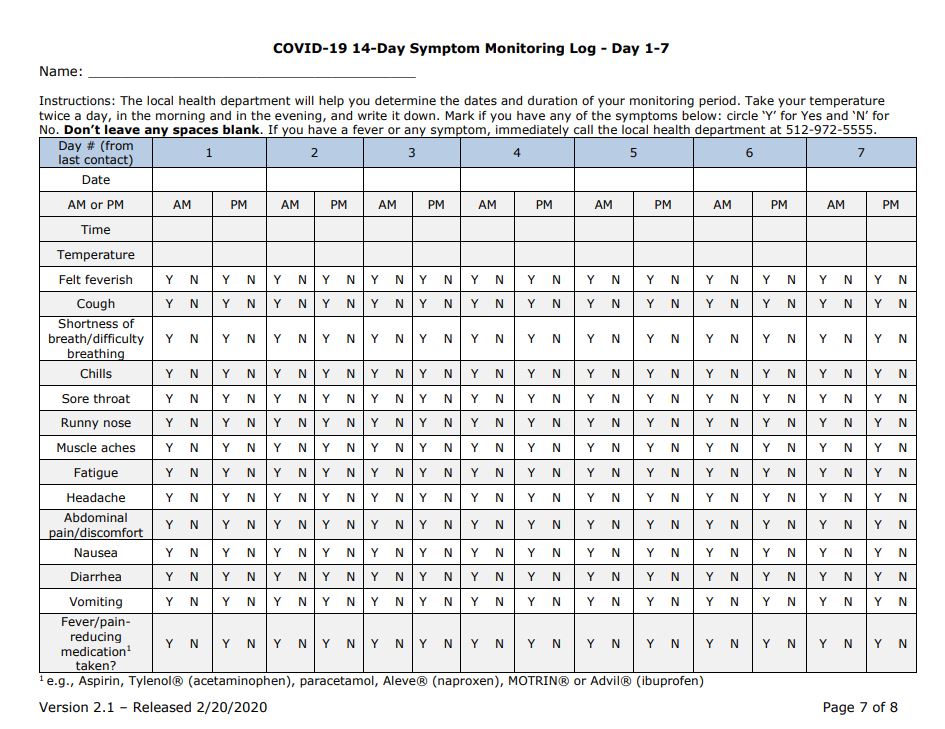
Your isolation can end when you meet ALL of the following criteria.
If you are symptom-free, you still should isolate for at least 10 days.
Here are two other important considerations:
Remember, the most important considerations are that you do what you can to prevent catching the disease and that you promptly get tested after a possible exposure. Waiting for symptoms is a bit too late.

This Straight, No Chaser looks at the African American community and the upcoming COVID-19 vaccine.

Indeed, the African American community specifically has decisions to make as we approach the possibility of a vaccine for Covid-19 being available. Here’s the thing. This community continues to be disproportionately affected by COVID-19 for reasons that have been previously discussed in this blog. As such, there is a significant amount of righteous angst about the social determinants of health and the institutional racism that play into why this has become yet another healthcare disparity.
However, the issues about the upcoming COVID-19 vaccine point to another issue begging to be addressed. I’ll support anyone who analyzes data and recommendations and after doing so, makes an educated decision not to accept the immunization. However, you can not think it’s rational to reject a potential lifeboat out of hand before even seeing the data. We fear the unknown and mock what we don’t understand. However, this is still America. We can still perform great feats in the face of crisis.
More importantly, think about what’s being said here.
So if you opt out, will you still complain about the health care disparities confronting our community on this issue? Also, how and when do our lesser choices become our failures of responsibilities? I understand distrust of the government. I’ve lectured on the Tuskegee experiments and healthcare disparities for years. Additionally, I’ve counseled and disciplined physicians discriminating against patients. That should not be our primary concern at this moment.
Furthermore, I also understand that education and empowerment are the way out, not over-reliance on the government.
How about this: can we reserve judgement until we at least see the data and hear the recommendations from the CDC, WHO, the American Public Health Association and the American Medical Association? Would the views of the National Medical Association, our oldest, largest and most esteemed organization of Black physicians move you? How about if Dr. Kizzmekia S. Corbett (pictured above) and her team develops or supports the vaccine?
Remember this: there’s shared sacrifice required here. An effective vaccine requires about 70% of the population to take it to sufficiently create herd immunity. More importantly, as long as herd immunity doesn’t exist, it is the African American community that will be most severely and disproportionately affected by the ravages of COVID-19.
Choices have consequences. Let’s choose wisely.




This Straight, No Chaser addressing the challenge of reopening schools during the COVID-19 pandemic.
America’s futility in addressing Covid-19 has left us with an unavoidable choice. We could fight our individualistic instincts and economic realities and attempt a restart along public health best practices, but our personal and governmental COVID-19 choices render that choice practically unavailable. As such, any success we have in normalizing life will be found while simultaneously fighting the virus. We are left to prioritize meaningful activities that need to be reengaged.
Put me on the record. It’s time for precollege students to be able to return to school (but by no means in the way you were used to – more on that later). For those of us whose rallying cry has been “follow the science,” here we go. Shall we focus on the opportunity and not the obstacles? Let’s begin with the American Academy of Pediatrics’ (AAP) policy position that it’s medically safe for children to return. Folks, this is not an insignificant declaration. The AAP is the medical organization most charged with safeguarding children.
This is based on two considerations. Children have both low infection and transmission rates. This sets the bar for what’s possible. Follow the science, remember? Perhaps even more importantly, there are scores of data relative to the current level of damage occurring by children not receiving the socialization skills obtained by schooling. Let’s be clear: kids of all ages and levels of native/baseline intelligence are being developmentally delayed as a result of the ongoing isolation. This by itself is creating a series of long-term consequences that must be factored into the equation. From the AAP President: “We know that children learn more in school than just reading, writing and arithmetic… They get social and emotional skills, healthy meals and exercise, mental health support and other things that you just can’t get with online learning.”
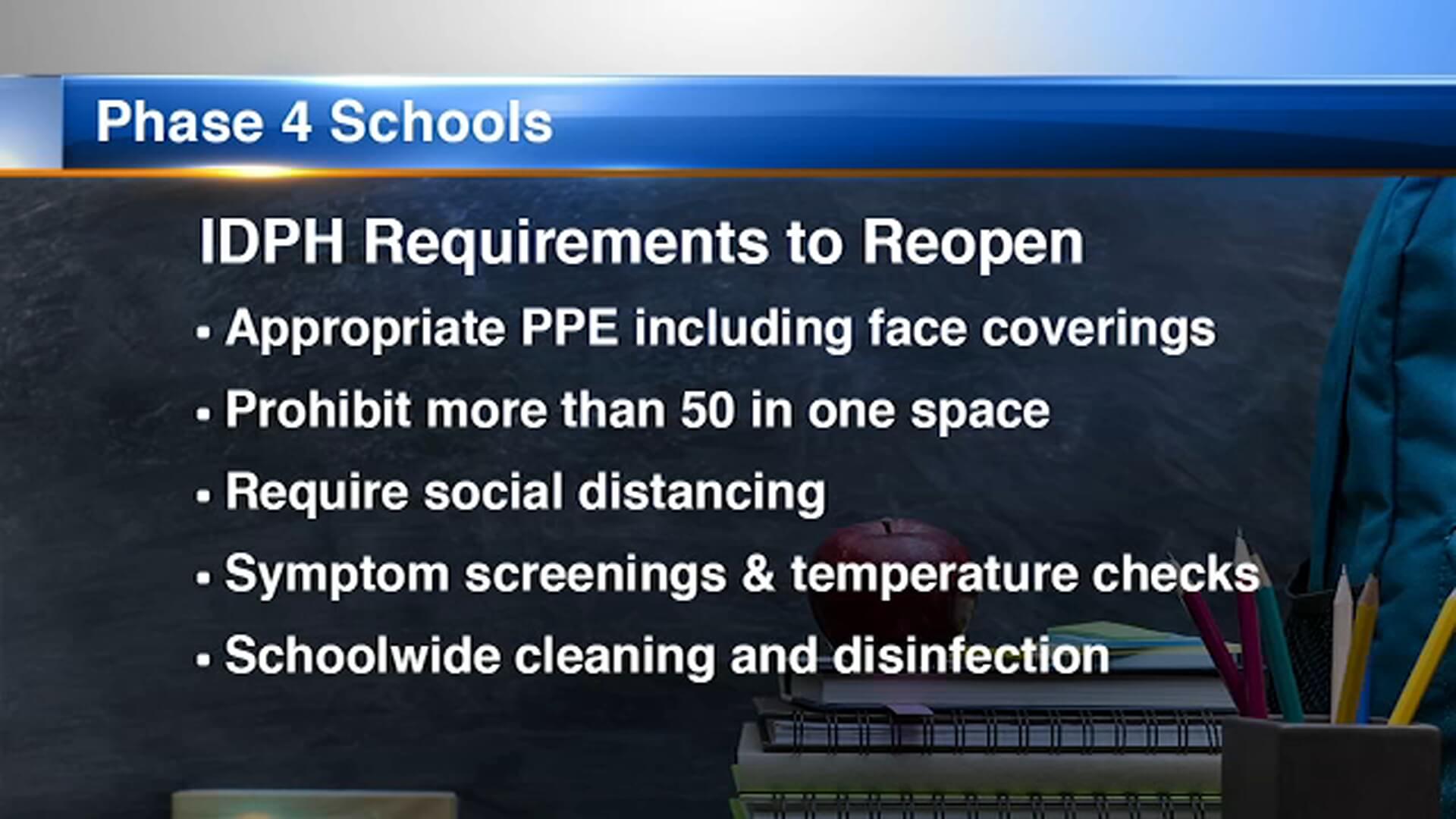
Thus, if the science states there is a rationale for children needing schooling, and it presents a relatively low threat to others, the obvious next question is “How can this be done safely, especially when considering teachers and others needed to operate schools who may be at heightened risk?” First, realize that there is a completely different question and set of considerations than the issue of whether children need to and can go back to school. The answers aren’t that difficult to fathom if you’d just avoid rejecting the premise out of hand. Consider the possibility if just these five considerations were fully implemented (shortened for the purposes of a briefer discussion).

It’s the American way to face our challenges, not cower from them. In this example, there are compelling reasons to have this group of essential workers perform an essential function for our children. The science suggests we can do so relatively safely if we meet the challenge with creativity. It’s time. The world has changed. We must adapt. I welcome your thoughts and challenge you to ask your schools which of these basic considerations have been accommodated. If you’re interested, here is a full list of CDC recommendations on the topic.

This Straight, No Choices address our COVID-19 choices. We’ve focused a lot on our failures getting the fundamentals of public health implemented, both nationally and within most states. However, let’s not be so smug as to believe all problems that have and will manifest are the problems of the political right. This is not to excuse but explain and warn. We still have a long way to go, and there’s not much indication that we’ve yet begun to get there. The data points in the wrong direction, and it’ll bleed into the next respiratory season with a trampoline effect on cases.
Americans treasure independence, free will and what’s left of what were our freedoms. As related to COVID-19, we all seem to have a line drawn as to where we won’t do what’s necessary to protect ourselves and the general population. It certainly is (but it’s not just) failure to honestly implement the Defense Production Act, to order a national shutdown, testing and contact tracing programs, holding rallies, persistent dishonesty about the data and reporting (I could go on…).

However, there’s more that we, the people, say and do every day, and there’s things we support that make no sense if the goal is to eliminate this virus. Here are a few.
If you think about the demographics of these activities, you’ll realize they encompass the full political spectrum and multiple demographics. Let’s just take one example. Everyone’s been awaiting the development of a vaccine, but if upwards of 70-75% of us don’t take it, it won’t produce a desired mass effect of reducing the viral load and producing herd immunity.
All of this leads me to conclude that the challenges of COVID-19 will continue for a long time. See, if we each have a line that’s drawn, we all will ultimately contribute to the ongoing and rising level of deaths. Americans have rights and individual freedoms, and you’re expressing them with your actions. Choices have consequences. Can you be as honest about that as we’re demanding our leaders be honest about what they aren’t willing to do? Are you ok with what that will mean for the foreseeable future?

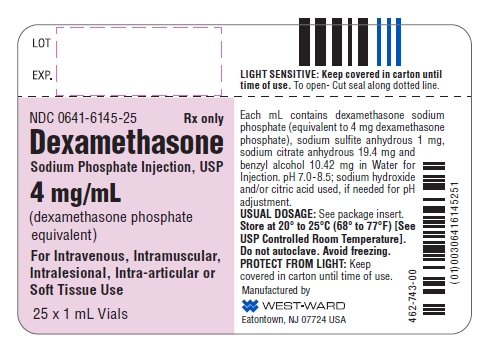
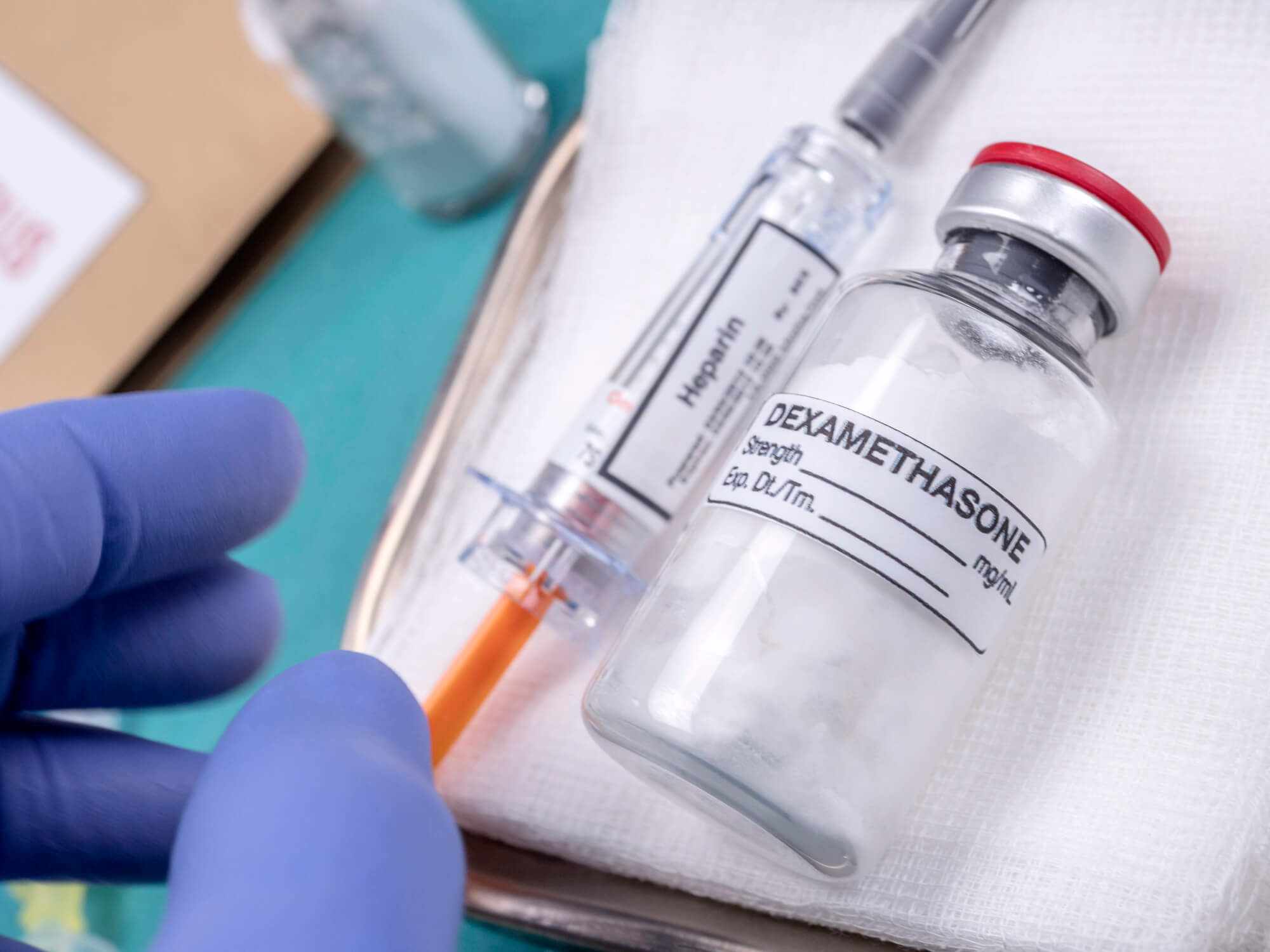 In the news, this Straight, No Chaser reviews new findings on the use of dexamethasone in treating COVID-19. Dexamethasone is a commonly used steroid that has sixty years of use behind it.
In the news, this Straight, No Chaser reviews new findings on the use of dexamethasone in treating COVID-19. Dexamethasone is a commonly used steroid that has sixty years of use behind it.

![]()




This Straight, No Chaser addresses how you can access safe church reopening strategies.
Between Sterling Initiatives and SI Medical Supply, we’re providing consulting and services for several houses of worship in anticipation of the time at which in-person services resume. Given the differences in each state and, in fact, each location, it is frankly irresponsible to offer a blanket set of recommendations as to how churches and other houses of worship should prepare beyond recommending adherence to CDC guidelines for reopening.
However, I’m always inclined to point out that it’s not just knowing what to do that creates success. Implementing best practices is what creates outcomes of interest. As such, Sterling Initiatives is offering the first fifty (50) houses of worship that reach out to us free consultation toward lowering the risks of Covid-19 infection. As time permits, we’ll do this through the end of the month. Are you or your house of worship is interested in discussing these steps? Reach out to us at 844-724-7754. You can also reach us at sterling@sterlinginitiatives.com.

We’ll discuss some of the following, at no cost to you:
We’re here for you. Be ready so you don’t have to get ready. Embracing safe church reopening strategies is a must. You don’t want to face the alternative.
#KnowledgeIsHealth #HealthSelfEmpowerment

This post addresses COVID-19 transmission from touching surfaces. Today’s advice to you is not to confuse the reporting of science with information. Huh? The screaming headline of the day is an important piece of scientific nuance. Covid-19 is less likely than thought (and just unlikely to be spread) via contact with surfaces. However…
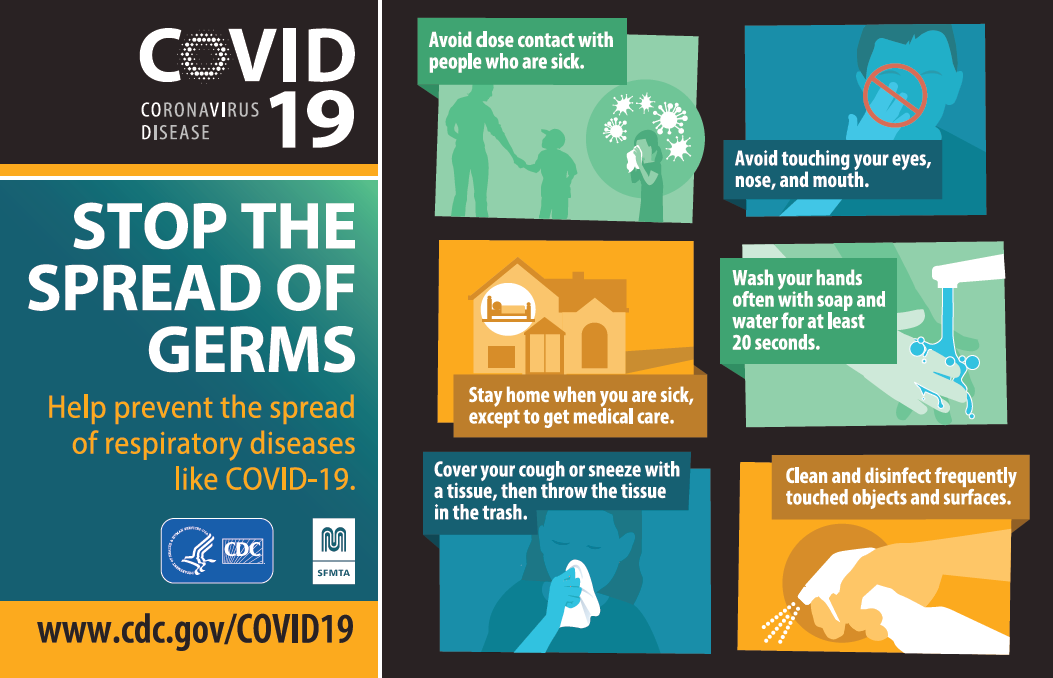
Now what are you supposed to do with this information? Unfortunately, low-information users will ignore the nuance and declare “America is reopen. It’s back to business as usual.” That would be an incorrect use of the information. Here are the appropriate take home points.




We are making choices. I asked people on my Facebook page if they would take a vaccine if approved and available this December. 89% said they would not. I asked if people would take hydroxychloroquine for COVID-19 prophylaxis. 99% said they would not. I asked if people would go back to work (not including remote work capabilities). 75% said they would not. Still, America is also in an economic crisis. Like it or not (and survive it or not), America is reopening. If you have the wherewithal to wait until an acceptable vaccine and treatment regimen is available with which you’re comfortable, or if you’re willing to survive on unemployment benefits, your decision is made. However, if you are inclined to roll the dice within a vaccine or effective treatment, you’d better be trying to optimize every other means of protecting yourselves.

Let’s consider this your simple personal COVID-19 reopening checklist as to how you reengage once you choose to.
What are you going to? Whatever your choice, be smart. Your choices have consequences and will affect others. Stay safe.


This Straight, No Chaser makes a call to adjust priorities within our healthcare system. Can we take a moment and reflect on how poorly designed our healthcare system is? If COVID-19 has done anything (besides killing over 80,000 Americans – and counting), it has shown us how our outcomes are the consequences of our choices and priorities. The American health care system is the world’s best at identifying and treating diseases and their complications. It is not nearly as good at promoting health and preventing disease. Clearly these last two considerations aren’t the same. Sadly, stressors like COVID-19 reveal how fragile our public health infrastructure is. The diseases display the limits of waiting for disease to appear to begin a response. This is true even before you address healthcare disparities, which exist between rural and urban areas, various ethnic groups and within socioeconomic classes. It’s time to stop just lamenting our current level of unpreparedness.

I again make a call for a revisiting of our public health system and placing health promotion and prevention on an equal footing has curative care considerations. This is consistent with the modern need for patients to assume more responsibility for their own care between physician visits. Prioritizing this level of activity also strengthens individuals for those times when diseases arise. The COVID-19 pandemic must be viewed as not a once in a lifetime pandemic as much as an examination of our system. It reveals real opportunities for improvement but for transformation of our healthcare system. It’s time for innovation.

It’s time to stop viewing the emergency room as an appropriate portal of entry into the healthcare system for over 20 million Americans. This leaves individuals presenting with advanced disease in imminent risk of death. How can that be viewed as an acceptable option? It’s time to start reprioritizing health as a way of life. We must weave the notion of health promotion into the fabric of society and have individual communities educated, engaged and empowered. Let’s stop playing games and politics with that which translates into length and quality of life. Let’s stop primarily viewing healthcare as a driver of 17% ($3.5 trillion) of the US economy and start viewing its delivery as a fundamental part of what it means to have a society.
![]()
How can it be viewed as a bad thing to have an infrastructure in place that allows us to stay ready instead of having to get ready. Imagine an America with a national infrastructure inclusive of personal protective equipment (PPE) already in a state of readiness, as we do with military bases? Why not have a national screening apparatus in place waiting to be deployed? Instead of just slotting emerging healthcare professionals into curative care professions, let’s prioritize the development of exclusively preventive care professionals. These initiatives amount to way more than ounces of prevention. This reconfiguration of healthcare provides jobs, better health care outcomes and a more efficient system all around. I have recently created an organization along these lines. America’s first managed preventive health care organization, named SIMPCO, will be addressing these challenges in communities around the world. Doing so successfully will allow us to better address spontaneous eruptions like COVID-19 when they arise without hundreds of thousands of excessive lives lost beyond the unavoidable. Much of what we need to be successful lies in the hands of individuals to know better, do better and thus, be better. The future is upon us. Knowledge is health.

This Straight, No Chaser features some of Dr. Sterling’s recent media appearances. View this, and get answers to many of your questions!

This Straight, No Chaser offers this week’s CDC COVID-19 Update.
All of this points out that things are still quite deadly but are slightly improving. Stay safe.


This Straight No Chaser addresses why testing for COVID-19 still matters.
We’ve diagnosed 1 million Americans with COVID-19. The US is testing at a rate of 16.4 tests per 1,000 people (Comparatively, Spain and Italy – the countries with the second and third highest number of cases – have tested 22.3 and 29.7 tests per 1,000 people respectively). We’ve only tested 4 million citizens overall, representing 1.2% of the population. Simply put, we want to reengage.
There are two approaches to this.
This isn’t even about stay at home considerations at this point in the conversation. The goal here is to impart some intellectual honesty into the conversation. The goal is to make sure you understand that what happens in the fall is contingent on what happens now. There obviously is an equivalent of willful ignorance occurring at the federal level. Not only do we not have a sufficient number of effective tests, but there are ongoing shortages of the materials needed to run these tests.
There has been no serious implementation of the Defense Production Act that would compel business to create what’s needed. Without testing, we won’t detect new infections. We can’t engage in contact tracing. We can’t have intelligent discussions about when communities specifically need targeted isolation.

The Rockefeller Foundation recommends expansion of the US testing capacity to 3 million tests per week for the next two months, followed by 30 million tests per week for the next six months. Yes, it’s calling for a marshaling of the nation’s resources to make this happen. It’s in the national public health and economic interest. Harvard has made a similar calling for ongoing testing.
Those would argue against vigorous testing at this point are not only being willfully ignorant but are contributing to the second wave of cases that will emerge in the fall. Forewarned is forearmed. If you live in one of the increasing places that are offering tests, please go get tested. It’s not just about you. Your apathy is directly contributing to the deaths of those most vulnerable. Know better. Do better. Be better.


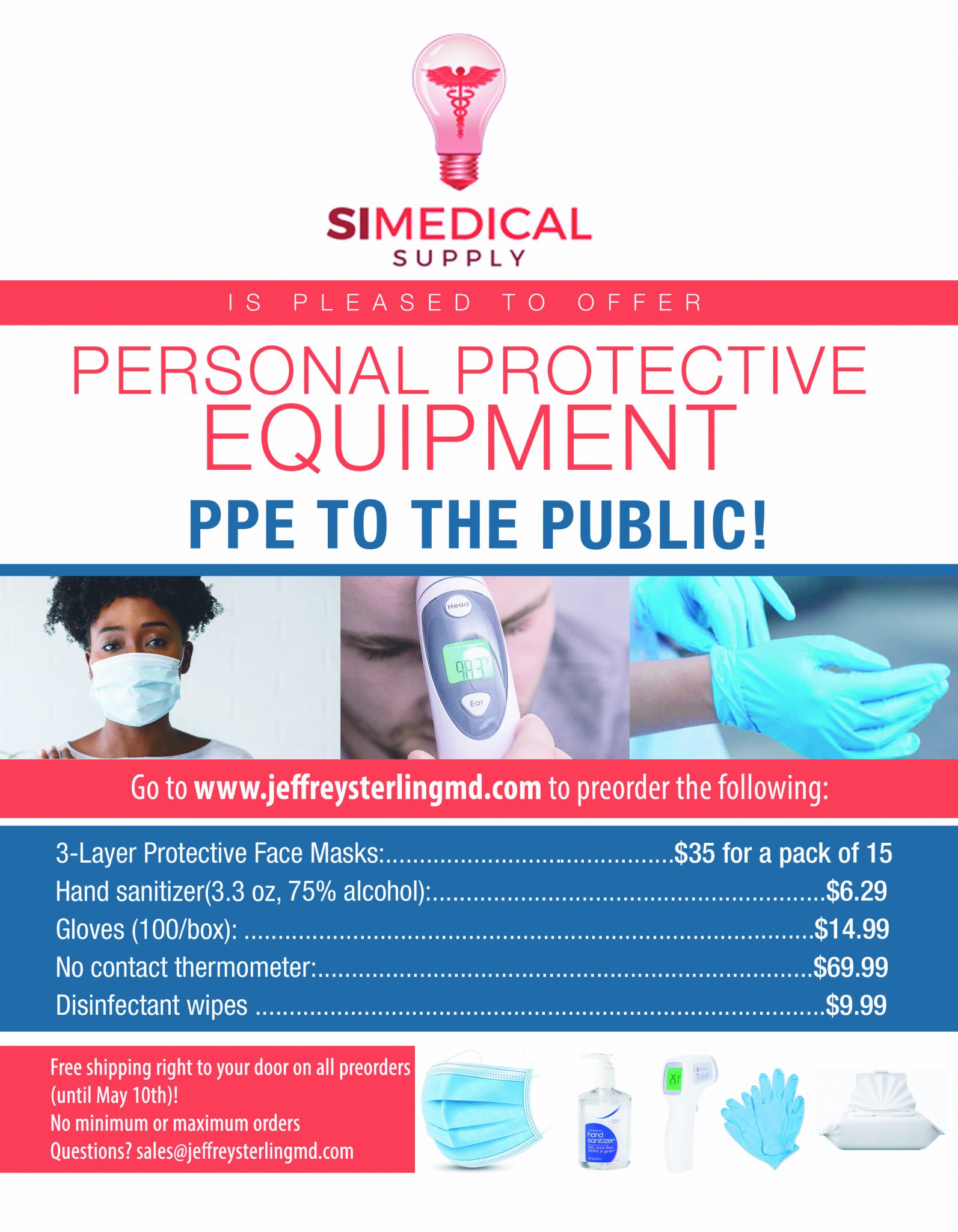
Act now! Secure your families and your health with the following.